




Federal and state regulators, along with policymakers, are actively amending network adequacy standards and provider directory accuracy requirements. These updates carry far-reaching implications for your organization and can influence how you manage networks, provider data, and compliance going forward. A thorough understanding of these network adequacy policy updates, provider directory compliance requirements, and provider data management trends will help you navigate what’s ahead and position your organization for success.
Medicare Advantage
The Medicare Advantage program continues to see policy changes aimed at improving provider directory accuracy, giving you new guidelines to follow. Two major updates impacting you are The Requiring Enhanced and Accurate Lists of Health Providers Act (REAL Health Providers Act) and the CY2026 Final Rule for Medicare Plan Finder (MPF).
New Medicare Advantage Provider Directory Accuracy Requirements
The Requiring Enhanced and Accurate Lists of Health Providers Act (REAL Health Providers Act)
The Requiring Enhanced and Accurate Lists of Health Providers Act (REAL Health Providers Act), part of the “Consolidated Appropriations Act, 2026,” sets new provider directory accuracy requirements for MA organizations. Starting with plan year 2028, you’ll be expected to comply with several new requirements for verifying provider data and updating your directories.
Key Requirements Under the REAL Health Providers Act
- Verify Provider Data Every 90 Days
- Indicate Unverified Providers in the Directory
- Remove Non-Network Providers from the Directory within 5 Days
- Verify More Provider Directory Information
- Conduct and Submit Annual Accuracy Analyses and Reports to CMS
- Display Provider Directory Accuracy Scores in MA Directories and on a CMS-Maintained Website *Starting Plan Year 2029
💡 If you’re involved in any part of this process, it’s important to understand the REAL Health Providers Act and its impact on your organization. To dive deeper into the new requirements, read our article: The REAL Health Providers Act Signed Into Law: New Provider Directory Accuracy Requirements for Medicare Advantage.
CY2026 Final Rule: New Provider Directory Requirements for Medicare Plan Finder
The Medicare and Medicaid Programs Contract Year 2026 Policy and Technical Changes to the Medicare Advantage Program Final Rule, brings additional requirements related to MA provider directories. Moving forward, you must submit provider directory data directly to CMS for integration into the Medicare Plan Finder (MPF) website—a centralized platform that helps Medicare beneficiaries compare and select health plans during the annual open enrollment period.
Key Requirements Under Format Provider Directories for Medicare Plan Finder
- Submit data to CMS/HHS for online publication in the Medicare Plan Finder.
- Submit or make the required data available in the specified format, method, and timeframe set by CMS.
- Update provider directory data within 30 days of becoming aware of any changes.
- Confirm annually that submitted or available information is accurate, following CMS requirements.
The Latest Medicare Advantage Provider Directory Requirements
Learn more about the updated Medicare Advantage provider directory requirements and what they mean for you.
Additional Network Adequacy and Provider Directory Accuracy Updates and Compliance Requirements
There’s more to be mindful of regarding provider data accuracy and network adequacy compliance.
Network Adequacy Applications and Submissions
- As part of initial applications and service area expansions applications, you must demonstrate compliance with network adequacy requirements a year in advance of your go-live date.
- If Letters of Intent are used during your initial or expansion network application process, you’ll have a Triennial Network Adequacy Review in the first year your plan is operational.
Triennial Network Adequacy Reviews
- Full network audits are still a staple of compliance. Read our article to learn more about the process and how to stay prepared: Triennial Network Adequacy Review Essentials for Medicare Advantage Organizations.
Behavioral Health Services Provider Activity Verification
- The focus on behavioral health services continues to grow. You must verify annually that listed behavioral health providers—including Physician Assistants (PAs), Nurse Practitioners (NPs), and Clinical Nurse Specialists (CNSs)—have provided services to at least 20 patients in the past year. Read more about these requirements in our article: Behavioral Health Policies in Medicare Advantage.
CMS Oversight and Compliance Activities for Medicare Advantage
You’ll find CMS oversight activities continuing through a range of efforts. These include online directory reviews, secret shopper surveys, ad-hoc audits, and other monitoring tools.
💡 If there’s one takeaway, it’s that preparation matters. You want to make sure you have everything for your network review. Prepare for your next network audit with our Medicare Advantage Network Adequacy and Provider Data Accuracy Audit Toolkit.
Marketplace and Exchanges
Qualified Health Plans (QHPs) offered through the Federally-facilitated Exchange (FFE), a State-based Exchange (SBE), and the State-based Exchange on the Federal Platform (SBE-FP) are seeing regulatory updates. CMS and the Center for Consumer Information and Insurance Oversight (CCIIO) continue to implement new policies that impact QHP Certification. These policies include changes to network adequacy evaluations, network adequacy provider data validations, and provider directory accuracy.
Federally-facilitated Exchanges
Network Adequacy Time and Distance Methodology
QHP network adequacy time and distance standards are evaluated using geographic distance calculations rather than estimated driving times. This methodology takes into account topographic barriers such as rivers, lakes, and mountains, which can influence how individuals travel to access care, as well as how health plans organize their networks to meet compliance requirements.
Alternative Time and Distance Standards
Additionally, Alternative Time and Distance (T&D) Standards for certain county-provider specialty type combinations where CMS has determined the baseline network adequacy time and distance standards cannot reasonably be met due to external factors, such as provider shortages or geographic barriers. For additional guidance, refer to the QHP certification webpage.
Network Adequacy Provider Validations
Network Adequacy Provider Validations remain a key component of the QHP Certification process and year-round compliance. For Plan Year (PY) 2027, you can expect the same network adequacy provider data validations that were introduced last year. These include limiting providers to a maximum of 10 practice locations, a new provider specialty framework, a new physician specialty compatibility matrix, and guidance on how to populate specific data fields.
💡 Learn more about the latest Network Adequacy Provider Data Validations in our Executive Summary: QHP Certification Data Validation Best Practices.
CMS Oversight and Compliance Activities
CMS and CCIIO conduct oversight activities throughout the year to assess issuer compliance with QHP certification requirements. These activities ensure adherence to Exchange-specific certification requirements and operational guidelines throughout the plan year.
Issuer Compliance Monitoring
Compliance monitoring is based on multiple state and national data sources, including:
- Complaints data
- Issuer self-reporting of problems
- Issuer policies, procedures, and operations
- Network adequacy analysis
- Indicators of customer service and satisfaction
Issuer Compliance Reviews
CMS may select your plan for a compliance review at any time during the year. In some cases, CMS works with state regulatory entities during this process. After compliance reviews are completed for the year, CMS provides issuers and states with summary findings and lessons learned. General findings are also made available to the public.
💡To learn more, visit the QHP Certification Compliance webpage.
Health Policy Update: Final Notice of Benefit and Payment Parameters for 2027
Zach Snyder, VP of Government Affairs at Quest Analytics, discusses the HHS Notice of Benefit and Payment Parameters for 2027. He explains the key changes to network adequacy and essential community provider standards, and what the updates mean for health issuers and states.
No Surprises Act
Provider Directory Verification Requirements
The No Surprises Act remains integral to healthcare policy by protecting your members from unexpected out-of-network charges and reducing unplanned expenses for your organization. It requires health plans, providers, and facilities to maintain accurate provider directories. To comply, health plans, providers, and facilities must work together to establish compliant provider data verification processes.
Additionally, health plans must establish processes for provider data management, directory maintenance, verification protocols, and member communications.
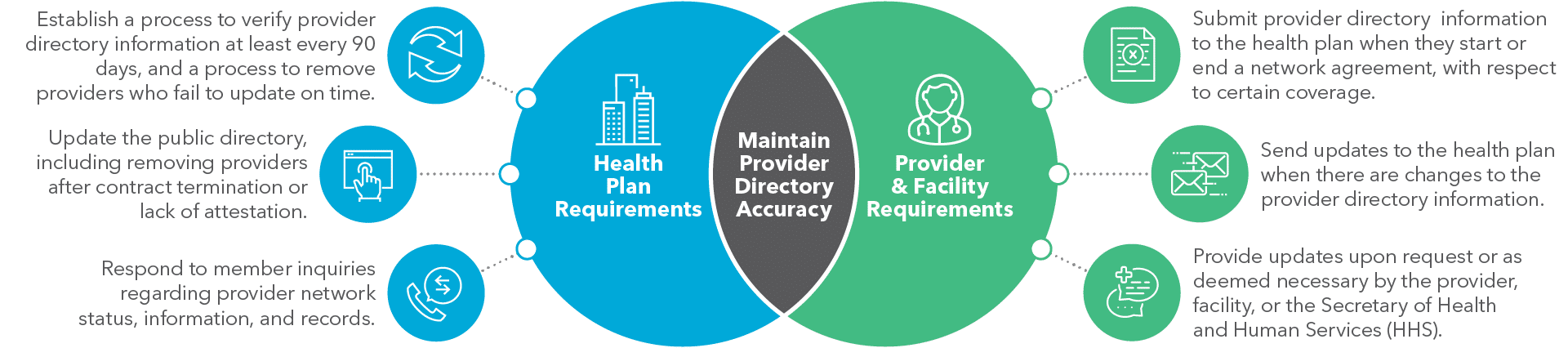
Payer and Provider Responsibilities
Medicaid
New Provider Data Accuracy Regulations
Medicaid and the Children’s Health Insurance Program (CHIP) are adopting standards closely resembling those applied to Medicare Advantage and Marketplace programs. You will see new requirements emphasizing provider outreach, provider data verification processes, and timely data updates.
The Consolidated Appropriations Act (CAA) and the Medicaid/CHIP Managed Care Access Final Rule have added provider directory accuracy requirements for Medicaid and CHIP. Programs are required to implement provider outreach and verification processes to meet directory accuracy requirements. These regulations align Medicaid and CHIP standards with those already applied to Medicare Advantage and Commercial plans. Applicability to Medicaid and CHIP Fee-for-Service (FFS) programs, Managed Care Organizations (MCOs), Prepaid Inpatient Health Plans (PIHPs), Prepaid Ambulatory Health Plans (PAHPs), and Primary Care Case Management (PCCM) entities.
Medicaid Provider Directory Requirements Common Themes
While specifics for Medicaid programs may vary, you’ll see several common requirements.
Quarterly and On-Demand Provider Data Updates: Provider directories are to be updated at least quarterly or more frequently, as required by the state and/or Secretary of Health and Human Services.
Provider Outreach and Verification Processes: Plans are required to develop and deploy provider outreach and verification processes to adhere to the new standards.
Verification of Specific Provider Directory Data Elements: This includes verifying provider contact information, specialty, cultural and linguistic capabilities, acceptance of new Medicaid patients, and network status.
Timely Updates to Searchable Electronic Provider Directories: A searchable, electronic provider directory must be updated no later than 30 calendar days after the plan entity receives updated provider information.
What to Watch: We expect to see more legislative changes that bring additional requirements for provider data accuracy, provider network auditing, and provider verifications in Medicaid programs.
2026 Emerging Provider Data Management and Provider Data Accuracy Trends
Provider data accuracy and network adequacy are in the spotlight as we move through 2026, bringing a mix of new data trends. Let’s take a closer look at what’s a priority for provider directories and network submissions.
Trend 1: Indicating Provider "Accepting New Patients" Status in the Directory
Indicating whether a provider is accepting new patients is one of the most sought-after updates for directories this year. Healthcare consumers want to know which in-network providers are actively taking new appointments, especially around Open Enrollment — and regulators are backing this expectation.
What The Regulations Say About Medicare Advantage
CMS requires that your MA provider directories make it easy for members to identify whether providers are currently accepting new patients. According to the Medicare Advantage and Section 1876 Cost Plan Provider Directory Model and Instructions:
“Clearly identify whether or not a provider is accepting new patients or provide a notice directing beneficiaries to contact a provider to determine if he or she is accepting new patients. Plans may identify providers who are/are not accepting new patients in any manner (i.e., “Accepting New Patients? Yes/No” or an “*” with a footnote), so long as beneficiaries can determine those providers from whom they may reasonably expect to obtain services.”
What The Regulations Say About Marketplace and Medicaid Plans
Marketplace and Medicaid programs have similar requirements for displaying a provider’s “accepting new patients” status as part of their core directory standards.
How You Can Stay on Trend
Incorporating “accepting new patients” status as a required data field in your provider verification processes can help bridge the gap between compliance and member satisfaction. Consider adding it to your outreach scripts, digital attestation portals, and data management workflows. Integrate this step into audit cycles to verify compliance and usability.
It’s also important to communicate to your contracted providers and provider groups that this status is mandatory and must be updated promptly whenever changes occur, especially during periods of high patient demand.
Trend 2: Listing Only Providers with an Active National Provider Identifier (NPI)
There’s a renewed focus on only listing providers who have an active National Provider Identifier (NPI), are in-network, and are actively seeing patients in your directories and network submissions – which means you want to have it on your priority list. Everyone involved is working toward the same goal: avoiding scenarios where members attempt to schedule an appointment with a provider who is no longer practicing, is out-of-network, is considered a ghost provider, or is on the Office of Inspector General’s (OIG) List of Excluded Individuals/Entities (LEIE).
What The Regulations Say About Medicare Advantage
Your MA provider directories can only include providers who have an active NPI and have a valid network contract, according to the CMS guidelines. Providers who don’t meet these criteria, such as those who have retired, passed away, have opted out of Medicare Advantage, or appear on the OIG’s LEIE list, must be excluded from your directories.
What The Regulations Say About the Marketplace
PY 2027 Network Adequacy Provider Validations mirror this idea but provide further clarification on what is allowed and not allowed for QHP certification and year-round compliance.
- NPIs Must Be Active and Verified in NPPES: During your QHP certification process, providers included in your network submission must have a valid and active NPI. If an NPI cannot be confirmed in the National Plan and Provider Enumeration System (NPPES), you will need to remove the provider from your Network Adequacy (NA) Template data to address validation errors flagged in the Marketplace Plan Management System (MPMS).
- Ongoing Monitoring for NPI Discrepancies: It’s worth noting that even after validation in MPMS, active NPIs may later be flagged as inactive or missing during subsequent reviews of NPPES data. Regular updates and monitoring are necessary to resolve these discrepancies.
- Removal of Providers on the OIG LEIE List: Providers on the OIG LEIE list can’t be included. If a listed provider is on the OIG LEIE, you must remove that provider from your network submission and directory data.
How to Stay on Trend
You’ll want visibility into which providers are at risk of non-compliance and the ability to understand the downstream effects of removing providers from your network data analyses and provider directories. Use dashboards that allow you to quickly identify providers with inactive or missing NPIs, ghost providers, providers who appear on exclusion lists, and providers who no longer meet participation criteria.
Before making any changes, use “what-if” scenario modeling to evaluate the downstream effects. Understand how removing these providers would impact network adequacy, access, performance, and other business priorities. By regularly reviewing the impact, you can minimize service disruptions and maintain a member-centric focus that balances compliance and network reliability.
💡For more quick tips on managing provider NPIs and directory data, download Best Practices for Managing Your Provider NPI Data.
Trend 3: Limiting Provider Location Listings to Where Care is Delivered
Location matters. When it comes to provider data, it’s important to list only the practice addresses where patients can reliably book appointments and receive care. Outdated or inaccurate practice locations continue to be a top error in directories. These inaccuracies can mislead patients and inflate the network size, causing you to lose visibility into the actual availability of care.
Regulators are paying increased attention to the issue of valid practice locations. New policies aim to establish clear definitions of “acceptable locations” to reduce discrepancies and ensure patients have access to reliable, accurate information in provider directories.
What The Regulations Say About Medicare Advantage
CMS provides the following guidance on practice location data:
- “List only the office or practice location(s) where the provider regularly practices and is regularly available to provide covered services.”
- “You may not list a provider if the enrollee cannot call the phone number listed and request an appointment with that provider at the address listed (e.g., urgent care or residential facilities; locations where the provider only has admitting privileges, only treats inpatients, or exclusively reads tests at the location).”
- “You may not list locations where a provider may practice only occasionally (e.g., locations where the provider is covering for other providers or locations within the practice where the provider does not regularly see patients).”
💡Note: Although CMS has not set a limit on the number of locations a single provider can be listed at, past reviews suggest 10–15 locations is typically considered reasonable.
What The Regulations Say About the Marketplace
Marketplace rules go a step further by setting a cap on the number of locations you can list for an individual provider.
- Under PY2027 Network Adequacy Provider Validations, “Issuers must not report more than 10 unique address locations for any one individual practitioner NPI or facility provider NPI.”
- “For purposes of network adequacy, CMS requires that an individual provider offer in-person services at the respective location a minimum of 1 day per week for that location to be entered by an issuer on its Network Adequacy (NA) Template as a unique location for that provider.” QHP Network Adequacy FAQs
How to Stay on Trend
Start by identifying providers with ten or more listed addresses, or you could use your regulatory requirement as the benchmark. Next, confirm which of the addresses are sites where the provider is regularly delivering care. Then, consider scenario modeling to understand how removing outdated or invalid addresses might impact your network. This step can help you get a sense of how changes to provider location data will affect network compliance, access, and performance.
Trend 4: Aligning Provider Specialties with their Active Practice
Listing a healthcare provider’s specialties and subspecialties with what they are actively contracted to deliver for the given network is gaining momentum as a key focus for provider data accuracy this year. Stakeholders need this information to be correct for various initiatives throughout the network lifecycle. Regulators are paying closer attention to instances of duplicated or mismatched provider specialty listings within your directories and network submissions.
What The Regulations Say About Medicare Advantage
According to CMS guidelines, your MA directories must reflect provider specialties and subspecialties according to their contracted role within your network.
“Clearly identify the capacity in which the provider is serving for that particular network (i.e., specialty and/or sub-specialty), even if the provider is credentialed in more than one specialty.”
Example: An internal medicine physician/oncologist, who does not practice as a Primary Care Physician (PCP), cannot be displayed as a PCP in the directories. Instead, they should only be listed under the category of the services they will be furnishing to enrollees as an in-network provider.
What The Regulations Say About the Marketplace
Marketplace rules use a provider specialty framework to clarify what qualifies and what does not. CMS uses qualitative checks in the MPMS Module to make sure you classify providers according to their true practice areas and specialties. Three components of the PY2027 Network Adequacy Provider Data Validations outline this information:
- NA Provider Specialty Framework
- NA Physician Specialty Compatibility Matrix
- NA Physician Subspecialty Compatibility Matrix
How to Stay On Trend
Treat provider specialty alignment as an ongoing provider data integrity priority. Use tools or specialized workflows to check provider specialty listings against contract details. Establish processes that allow you to monitor updates and changes efficiently. Lean on regulatory guidelines like MA or Marketplace frameworks to influence your specialty classifications for network submissions.
Trend 5: Preparing for More Publicly Accessible Provider Data
As provider data becomes more publicly visible, it’s important to view it as an integral part of your brand reputation, network marketability, and network strategy. Maintaining accurate data directly reflects your network’s credibility and appeal, serving as a public indicator of its strength and quality, ultimately enhancing its attractiveness to prospective patients, partners, and stakeholders.
How to Stay On Trend
Create readiness across your organization. Start by evaluating your current processes—identify what’s working and what needs improvement for managing updates and corrections. Leverage automation and enterprise solutions because keeping up manually is no longer feasible. From provider outreach and attestation to real-time updates reflected in your data and network analysis, automation creates opportunities for efficiency and scale. By streamlining updates and simplifying data sharing, you can maintain accurate provider data that not only supports operational excellence but also elevates your network’s market appeal in the competitive healthcare landscape.

Is your provider data ready for these trends? Evaluate how your process measures up with our Provider Data Accuracy Assessment Toolkit. Download Now!
5 Provider Data Management and Provider Data Accuracy Trends That Are Here to Stay
While new trends are emerging, some essentials never go out of style. Five provider data accuracy and data management trends from 2025 remain essential in 2026.
Trend 1: Verifying Provider Data More Frequently
If you haven’t reviewed your provider verification process recently, now is the perfect time to do so. MA, Marketplace, and Medicaid programs require verification of provider data every 90 days, moving away from the previous language that referred to once-a-quarter updates. Beyond adhering to the 90-day cycle, regulators also expect updates whenever provider data changes are communicated or identified, not just during routine verification cycles.
How to Stay On Trend
You want your provider data accuracy process to balance predictable outreach with flexibility for real-time updates. Adopting a rolling 90-day outreach approach can help you verify provider details consistently and avoid gaps. It can also be useful to track responsiveness and address overdue updates as they happen, making the entire process more manageable.
Trend 2: Maintaining Audit-Ready Network Analytics and Reports
Audit readiness isn’t going anywhere. In fact, regulators and internal leaders are asking for more analytics and metrics on your provider outreach activities – and in this data-driven world, that shouldn’t come as a surprise to anyone.
Regulators want this information as evidence that you’re actively engaging providers and have a process for maintaining accurate network data. Leadership is equally invested in understanding whether your efforts are producing measurable results.
How to Stay On Trend
Having certain analytics readily available can strengthen your position and help you respond to both regulatory and internal requests.
Examples of Audit Analytics You Need
- Provider Outreach Activities: Analytics on provider interactions, such as when outreach occurred and the methods you used.
- Provider Responsiveness Metrics: Analytics on how providers responded, the method, and the timeframe of their responses.
Consistently capturing and maintaining this information strengthens your ability to present a defensible process. It demonstrates your ongoing efforts to verify, update, and maintain accurate provider data.
💡Tip: Quest Enterprise Services® (QES®) Accuracy provides additional metrics to help you monitor provider outreach activities. Read our blog for the details!
Trend 3: Reducing Turnaround Times for Provider Updates and Communications
Shorter turnaround times for updating provider information and sharing network changes continue to be a priority. Over the past year, regulators have rolled out tighter deadlines to reduce the time between receiving provider updates and making that information publicly visible.
For example, 2-day turnaround timelines to update directory information on websites and 5-day turnaround timelines to inform patients about network changes.
How to Stay On Trend
With tighter timeframes in play, it’s worth reviewing your process for notifying members about network changes and updating provider directories within regulatory deadlines. Taking a closer look at how you collect, validate, and apply provider data could help identify inefficiencies and create opportunities to streamline. Incorporating tools like APIs to connect systems and automation to reduce manual effort could improve efficiency and make meeting those deadlines a lot easier.
Trend 4: Annual Provider Directory Accuracy Improvement Targets
You’ll continue to see attention on year-over-year directory accuracy improvements. Incremental improvements are a measurable metric for both compliance and organizational success. Whether regulators require an annual increase in directory accuracy or executives want proof that network data is becoming more reliable, sustained incremental changes are central to long-term strategy.
How to Stay On Trend
Set specific goals to improve data error types that matter most to members, regulators, and your organization. Small, achievable wins will help move the needle without overwhelming your team.
💡 Tip: Use dashboards to visualize trends across your network and provider data. These tools make it easier to track progress and identify areas where further action is needed.
What to Watch For
As your data accuracy improves, you may see new network adequacy gaps. The relationship between provider data accuracy and network adequacy is nuanced but manageable. Check out our article to learn more about addressing these challenges and maintaining a balanced strategy.
Trend 5: Incorporating Claims Data to Identify Inactive Healthcare Providers
Regulators continue to explore adding claims data to existing provider directory accuracy requirements to help identify inactive providers within your network. This requirement expands upon the existing provider directory accuracy regulations instead of replacing them.
Regulatory Examples:
- Medicare Advantage Behavioral Health Verification Requirements: These require annual validation that behavioral health providers have treated at least 20 patients in the last year.
- State Examples: Illinois, Oklahoma, New Mexico, and Massachusetts have similar requirements.
How to Stay on Trend
Integrate claims data into your provider data maintenance processes as an additional point of validation. Claims data can act as a valuable signal when determining provider activity levels, especially for providers who haven’t recently attested or updated their information. By identifying those with little to no claims activity, you can better ascertain potential inactivity or shifts in practice status. Combine this insight with other verification methods to guide outreach efforts—confirming their status as active practitioners, network participants, or candidates for deactivation in member-facing systems. Leveraging claims data as part of a multifaceted strategy will not only enhance directory accuracy but also help ensure compliance with emerging regulatory standards.
Provider Directory Policy FAQs
What are the requirements for maintaining provider directories?
Health plans must maintain accurate and accessible provider directories in both digital and print formats. Online directories should be user-friendly and up to date, while printed directories must include the last updated date and direct consumers to the plan’s website to verify current provider participation.
How often must provider directory information be verified?
Health plans are required to verify and update provider directory information at least every 90 days for all contracted providers and facilities, whether the relationship is direct or indirect.
What happens if a provider does not verify their information?
If a provider or facility fails to confirm their information within the required timeframe, they must be removed from the directory until their details are verified and updated.
How quickly must provider directory updates be made?
Any changes submitted by providers or facilities, such as new information or network status updates, must be reflected in the directory within two business days. This includes removing providers who are no longer in-network.
How fast must health plans respond to consumer inquiries about provider status?
Health plans must respond to consumer questions about whether a provider is in-network within one business day.
Where can I find strategies for improving provider data compliance?
For more guidance on provider data management best practices and compliance strategies for the No Surprises Act, read our article Provider Data Management Tips to Successfully Meet the No Surprises Act.
Takeaways for Healthcare Organizations
When you look across these trends, you’ll notice a shared theme: you’re being asked to move from static, compliance-driven management to dynamic, member-centered information stewardship. These trends collectively serve a greater purpose to improve how you support people when they need care.
As you go forward, think of your efforts as a bridge connecting regulatory requirements, member experiences, and business goals. Regulations give you the floor, providing clarity on what must be done to remain compliant. Member experiences represent the ceiling, offering opportunities for innovation and personalized care. Your daily work brings these elements together, closing the gap between what must be done and what can be achieved.
By focusing on these trends and aligning your efforts with the needs of the people you serve, you pave the way for stronger connections, smarter networks, and better outcomes.
Elevate Your Provider Data Accuracy with QES Accuracy
Discover how Quest Enterprise Services® (QES®) Accuracy can make a difference. Our comprehensive solutions enhance your process, offer better data transparency, reduce ghost networks, and improve compliance. Empower your organization to excel in the evolving healthcare landscape. Learn more about Quest Enterprise Services® (QES®) Accuracy today!



Know Your Data, Grow Your Business
Get a complimentary strategy session with a Quest Analytics expert to learn how we can help you maintain network adequacy, improve data accuracy and achieve astonishing efficiencies.